Rezidivraten
after radical prostatectomy, radiotherapy and brachytherapy are high – but why?
Many patients, as well as doctors, believe that prostate cancer that has not broken through the capsule of the prostate is healed by the surgical removal of the prostate. On the surface, a logical concept. Because as long as the cancer is only inside the prostate, yes it should be completely removed from the patient’s body after the prostate is removed.
Biologically, this is nonsense, based on a lack of knowledge of microanatomy and tumor biology.
First of all, the proof that this is a misconception. The Brady Urological Institute of Johns Hopkins University provides the so-called Han Tables (named after Misop Han) on their website. These specify the recurrence rates after radical prostatectomy
Looking at the HAN Tables, we find that recurrence rates after radical prostatectomy are high even when the tumor was completely removed along with the prostate (“organ-confined disease” category).
So where do the recurrences in these cases come from? They originate from individual tumor cells that have migrated out of the prostate along connective tissue structures, lymphatic and blood vessels and have become embedded in the connective tissue surrounding the prostate. In fact, the tumor cells also circulate in the blood and can be detected there by means of a liquid biopsy.

This is because the prostate capsule is permeable to cells as it consists only of compacted connective tissue fibers. This can be imagined roughly like the edge of a forest:
From a distance of 1 km the edge of the forest looks like a wall, if you stand right in front of it you will notice that it is mainly made of air, with a few branches and tree trunks in between.
Accordingly, most recurrences after prostatectomy occur in the connective tissue that surrounded the prostate – and surrounds the prostate analogs after prostate removal.
So, strictly speaking, any prostate cancer treatment is just tumor mass reduction – the destruction or removal of the tumor mass IN the prostate. Tumor cells OUTSIDE the prostate remain in the body. This can be killed by the body’s own immune system. The patient is then cured – by his own immune system.
Radiotherapy gives tumor cells a chance to survive
While radical prostatectomy removes all tumor cells located in the prostate along with the prostate from the body, radiation therapy has a stochastic effect. This means that all cells in the irradiation field will only die if sufficient radiation-induced damage occurs in all of them.
This is a random process. From a purely statistical point of view, it is possible that not enough radiation damage occurs in individual cells or that this damage is repaired by the cell – in which case the tumor cell survives.
This fact is supported by the observation that recurrence-free survival increases with higher radiation doses1.
NanoKnife
A revolution in the treatment of prostate cancer
Once prostate cancer has been diagnosed, most patients are faced with a choice: Either surgical removal of the prostate (radical prostatectomy) or radiation therapy. Both procedures are fraught with significant side effects: Impotence and incontinence.
However, they by no means guarantee a cure: in most cases, prostate cancer comes back after surgery or radiation, as so-called recurrences are frequent (HAN Tables, Johns Hopkins).
Irreversible electroporation (IRE) treatment can avoid side effects such as impotence and incontinence with comparable efficacy
While modern, gentle treatments have long since become established in other areas of medicine, they are still a long time coming in urology. For breast cancer, the entire breast has not been amputated for a long time, but the tumor is removed focally. In renal cell carcinoma, if possible, not the entire kidney is removed, but only the tumor – the healthy part of the kidney is preserved. The prostate is still removed “radically”, i.e. completely, in most cases unnecessarily.
This has changed since the successful introduction of Irreversible Electroporation (IRE) for the treatment of prostate cancer. With IRE, prostate cancer can be focally destroyed, with a lower likelihood of side effects.
Our most important message: don’t be pressured into treatment. At VITUS we inform you in detail about all treatment options
Prostate cancer often progresses slowly. In most cases, you will have enough time to learn about all treatment methods. In addition, classical “radical” therapy (surgery and/or radiation treatment) rarely prolongs life expectancy in low-aggressive prostate carcinomas – and in highly aggressive carcinomas, according to available statistics, it does not do so in many men. The same applies to radiation therapy.
At the same time, the classical treatments lead mainly to serious side effects, rarely to cure: in 70-80% of all men erectile dysfunction occurs after surgery, in 20-50% of patients urinary incontinence.
VITUS Salvage-IRE and Salvage-ECT of Prostate Cancer Recurrences and Metastases.
In the VITUS PRIVATKLINIK we have specialized in the treatment of prostate cancer recurrences in recent years.
We find that established methods, such as radiation therapy, salvage prostatectomy, and antihormonal therapy, are not optimal treatment choices for many men with recurrences – and metastases – after prostate cancer.
Precision crucial for therapeutic success with NanoKnife
Since 2007, the IRE technique has been approved by the FDA in the USA and CE marking in Europe. This was done because corresponding studies prove that all cells within the treatment area can be killed with this method. In order to achieve this and carry out a successful IRE treatment, two factors are crucial:
- Firstly:
The exact position of the tumor must be known before treatment. - Secondly:
The treatment field must be placed in exactly the right position.
The first condition is fulfilled by multiparameter MRI examination, 3D biopsy and, if necessary, other procedures. The second condition is fulfilled by a minimally invasive procedure under general anesthesia. Sterile needles with variable exposure length are inserted. “Exposure length” refers to the area of the needle that exposes the tissue to electrical current. We have experience with this procedure since 2011 and have performed the most prostate treatments worldwide. This makes us one of the leading experts worldwide, while other clinics are just getting started.
What is the procedure of a NanoKnife treatment?
This step is perhaps the most important. NanoKnife is a focal, image-guided treatment whose results are only as good as the planning and diagnostics that precede it. This is because NanoKnife itself does not detect where the cancer is located.
As a patient, you should not compromise on diagnostics. All variants of ultrasound (including elastography and contrast-enhanced ultrasound) as well as rectal punch biopsies have alarmingly low detection rates. It is very unlikely that this will find (all) tumors.
At the present time, only multiparameter MRIs performed by specialized radiology institutes provide adequate imaging diagnostics – together with PSMA/choline PET/CT if required.
The 3D images from MRI are given yet another layer by a 3D saturation biopsy. We are specialized in both procedures. Both are required to achieve the diagnostic accuracy necessary to effectively deliver NanoKnife treatment.
Once our physicians and physicists have determined the target area using the MRI cross-sectional images and, if necessary, calculated it in advance using 3D simulations developed by us, the target area is saved and transferred to the surgical monitor on the day of the operation.
For prostate treatment, the needles are inserted transperineally, through the perineum (the area between the genitals and anus). An endorectal ultrasound helps with placement. Experience plays a decisive role here. Even two needles place high demands on the spatial imagination of the surgeon. Placements with many needles are extremely challenging. This is because the prostate is a relatively small organ with a complex geometry, surrounded by many sensitive anatomical structures. In addition, the positioning options of the needles are very limited. This process can sometimes take several hours, although here at the VITUS Prostate Center computer programs help us achieve the perfect placement.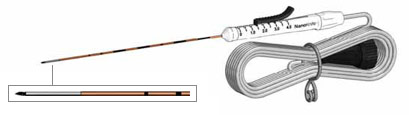
Figure 1: Minimally invasive NanoKnife electrode
Once the needles are precisely placed, their position is measured by ultrasound and passed on to the NanoKnife software and other external software. The area to be treated can still be adjusted on the computer by various parameters such as voltage, pulse duration and number of pulses. When all settings match the geometry of the prostate and tumor (always allowing for a safety margin around the tumor), NanoKnife charges its capacitors.
A potential difference builds up between each set consisting of two needles each. This is normally 3000 volts (V). This means that there is +1500 V on needle 1 and -1500 V on needle 2. The patient remains at 0 V. These voltages may seem more life-threatening than gentle, but their duration of action is in the range of millionths of a second. This makes the procedure safe and side effects such as burns are avoided. For more on the technology and the theory behind it, read more about the theory of IRE here.
The number of needles may vary and depends largely on the area to be treated. The computer of the NanoKnife system takes over the appropriate control of the needles, according to the previous settings. The treatment itself usually takes only seconds, a few minutes at most.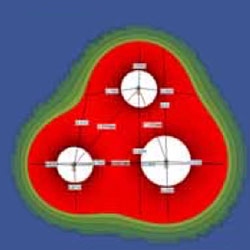
Figure 2: Precise planning of IRE treatment
Immediately after the needles are pulled out, the puncture sites close again. Most patients do not experience pain. However, some find the bladder catheter that is placed prior to treatment uncomfortable. It can be removed after 10 to 14 days. Small amounts of blood may still be found in the urine or seminal fluid several weeks later. This is because it takes up to six months for the body to move the tissue destroyed by NanoKnife ablation out of the body.
