NanoKnife
A revolution in the treatment of prostate cancer
Men diagnosed with prostate cancer are usually given the choice by their urologist to have the prostate surgically removed(radical prostatectomy – RPE) or to undergo radiationtherapy (radio therapy – RT). Both procedures are fraught with significant side effects: Impotence and incontinence are the rule.
However, they by no means guarantee a cure: in most cases, prostate cancer comes back after surgery or radiation, because these so-called recurrences are very common in prostate cancer.
Irreversible
Elektroporation (IRE)
NanoKnife treatment:
Highly effective, few side effects
This has changed since the successful introduction of Irreversible Electroporation (IRE) for the treatment of prostate cancer.
With IRE, prostate cancer can be focally destroyed, with a lower likelihood of side effects.
The broad spectrum of
IRE treatments:
From focal therapy to problem solver in unresectable T4 carcinoma.
IRE – also known by the product name NanoKnife – enables the gentle treatment of prostate cancer while avoiding impotence and incontinence.
IRE can be used to treat the full range of prostate cancers – from small focal carcinomas to T4 tumors that have already infiltrated the bladder or rectum – in other words, inoperable, usually advanced cases1.
Call us now on +49 (0)177 23 82 863 or get in touch using the contact form
Our most important
message: Do not allow yourself to be pressured into treatment.
At VITUS we inform you in detail about all treatment options
Prostate cancer often progresses slowly. In most cases, you will have enough time to learn about all treatment methods. In addition, classical “radical” therapy (surgery and/or radiation treatment) rarely prolongs life expectancy in low-aggressive prostate carcinomas – and in highly aggressive carcinomas, according to available statistics, it does not do so in many men. The same applies to radiation therapy.
At the same time, the classical treatments mainly lead to serious side effects, rarely to cure: 70-80% of all men experience erectile dysfunction after surgery, and about 20-50% of patients experience urinary incontinence: about 20% of men experience severe incontinence requiring several diapers per day, and an additional 30% experience moderate incontinence where one diaper per day is sufficient (see Table 1).
RT
3.2%
4.4%
9.4%
RT
60.8%
71.9%
93.9%
bowel function
RT
34.0%
31.3%
35.8%
Table 1: Long-term sequelae of radical prostatectomy (RPE) and radiotherapy (RT) for prostate cancer regarding incontinence, impotence, and impaired bowel function. Table translated into German. Resnik MJ, Koyoma T, Fan K-H, et al. N Engl J Med 2013; 368:436-45.
Irreversible electroporation (IRE):
The NanoKnife process
The NanoKnife tissue ablation procedure is a new type of therapy that is more than 10 years old and uses the irreversible electroporation (IRE) method to destroy cells. The surrounding tissue is not damaged in the process. Prostate cancer can be treated for the first time with this method in such a way that continence is preserved and there is only a low risk of impotence. In addition, the NanoKnife procedure has a very low likelihood of pain or scarring.
Here at VITUS, we are proud of the pioneering work we have done with the NanoKnife process. We are among the world’s leading experts in the use of IRE in the treatment of prostate cancer.
Through our close collaboration with the inventor of IRE for medical purposes, Prof. Boris Rubinsky of the University of Berkeley in the USA, we have had the opportunity to study and understand IRE at all stages of development, from laboratory to animal studies to human application. Our physicists and physicians are thus among the pioneers and world’s leading experts in electroporation processes – both in the scientific-technical field and in clinical use.
ADVANTAGES OF THE
NANOKNIFE TREATMENT
AT A GLANCE:
- One time treatment in only one day
- Highest potency retention rate achieved to date*.
- Statistical 0% Incontinence**, ***
- No surgical incisions
- No aftercare necessary
- No higher recurrence rate than radical procedures**.
- Treatment even after prostatectomy or radiotherapy
- Secondary immunological effects
* Urinary incontinence is the lack or inability of the body to safely store and self-directly empty the contents of the bladder. This leads to involuntary loss of urine. While there are several possible definitions of incontinence, a long-term study of incontinence after prostatectomy** concludes that a reasonable definition of incontinence is when a patient requires 2 or more pads per day 12 months after prostate surgery.
** Sacco E, Prayer-Galetti T, Pinto F, et al. Urinary incontinence after radical prostatectomy: incidence by definition, risk factors, and temporal trend in a large series with a long-term follow-up. BJU Int. 2006;97:1234-41.
*** Syan, Raveen, and Victor W. Nitti. “Post-prostatectomy Incontinence Initial Evaluation.” Urinary Dysfunction in Prostate Cancer. Springer, Cham, 2016. 15-30.
NanoKnife technology – ideal for the treatment of prostate cancer
The NanoKnife process is based on ultra-short pulses that generate strong electric fields. The pulses are 100 microseconds long – i.e. 0.0001 seconds. Compared to standard procedures, this new technology has unique features that make it ideal for treating the prostate.
- Tissue selectivity: Only cells that have a cell membrane, such as cancer cells, are reliably destroyed. All other structures, such as nerves, blood vessels and connective tissue structures, remain intact.
- Ultrasharp edges: With NanoKnife, the area between completely removed and untreated tissue can be measured in micrometers. This clearly sets NanoKnife apart from other treatment methods, such as radiation therapy, heat-based treatments and even surgery. In these methods, the central treatment field is always surrounded by an area where the tissue is unintentionally damaged. Often this is a zone with a diameter of several centimeters.
- Programmed cell death: NanoKnife causes cell death (apoptosis) to occur without causing radiation damage or burns and without forming scars. Current standard methods, such as radiation therapy (proton therapy, brachytherapy, etc.) and heat therapy (HIFU, microwave therapy, etc.), always create a large “toxic” area because the burned tissue is toxic to the body. The result is inflammation and pain with subsequent scarring. All of this prevents or limits further treatments that may be needed in the event of a recurrence.
- Repeatable any number of times: Since IRE treatment does not lead to long-term tissue damage, all other treatment methods (radiotherapy, heat, surgery) can continue without restriction after NanoKnife treatment. In addition, treatment using IRE can be repeated as often as necessary.
- Painless and minimally invasive: because no tissue is damaged by burning or radiation. In addition, only thin needles are used as invasive instruments. Thus, our patients usually hardly notice the treatment.
- Fast and in one session: Even extensive areas can often be treated under general anesthesia in just one session.
- Wide range of possible applications: The treatment of small, early detected prostate tumors is definitely the simplest application of NanoKnife. However, NanoKnife is also a treatment option for inoperable carcinomas that have already breached the prostate capsule, as well as for the treatment of recurrences that occur after radiation therapy, radical prostate removal, HIFU or brachytherapy.
- Immune system: The tumor fragments released during NanoKnife treatment support the patient’s immune system in fighting further tumors.
Precision is
crucial for the success of
therapy with NanoKnife
Since 2007, the IRE technique has been approved by the FDA in the USA and CE marking in Europe. This was done because corresponding studies prove that all cells within the treatment area can be killed with this method. In order to achieve this and carry out a successful IRE treatment, two factors are crucial:
- Firstly:
The exact position of the tumor must be known before treatment. - Secondly:
The treatment field must be placed in exactly the right position.
The first condition is fulfilled by multiparameter MRI examination, 3D biopsy and, if necessary, other procedures. The second condition is fulfilled by a minimally invasive procedure under general anesthesia. Sterile needles with variable exposure length are inserted. “Exposure length” refers to the area of the needle that exposes the tissue to electrical current. We have experience with this procedure since 2011 and have performed the most prostate treatments worldwide. This makes us one of the leading experts worldwide, while other clinics are just getting started.
Call us now on +49 (0)177 23 82 863 or get in touch using the contact form
What is the procedure of a NanoKnife treatment?
This step is perhaps the most important. NanoKnife is a focal, image-guided treatment whose results are only as good as the planning and diagnostics that precede it. This is because NanoKnife itself does not detect where the cancer is located.
As a patient, you should not compromise on diagnostics. All variants of ultrasound (including elastography and contrast-enhanced ultrasound) as well as rectal punch biopsies have alarmingly low detection rates. It is very unlikely that this will find (all) tumors.
At the present time, only multiparameter MRIs performed by specialized radiology institutes provide adequate imaging diagnostics – together with PSMA/choline PET/CT if required.
The 3D images from MRI are given yet another layer by a 3D saturation biopsy. We are specialized in both procedures. Both are required to achieve the diagnostic accuracy necessary to effectively deliver NanoKnife treatment.
Once our physicians and physicists have determined the target area using the MRI cross-sectional images and, if necessary, calculated it in advance using 3D simulations developed by us, the target area is saved and transferred to the surgical monitor on the day of the operation.
For prostate treatment, the needles are inserted transperineally, through the perineum (the area between the genitals and anus). An endorectal ultrasound helps with placement. Experience plays a decisive role here. Even two needles place high demands on the spatial imagination of the surgeon. Placements with many needles are extremely challenging. This is because the prostate is a relatively small organ with a complex geometry, surrounded by many sensitive anatomical structures. In addition, the positioning options of the needles are very limited. This process can sometimes take several hours, although here at the VITUS Prostate Center computer programs help us achieve the perfect placement.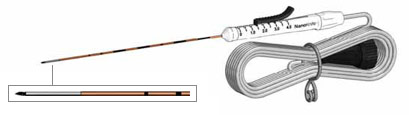
Figure 1: Minimally invasive NanoKnife electrode
Once the needles are precisely placed, their position is measured by ultrasound and passed on to the NanoKnife software and other external software. The area to be treated can still be adjusted on the computer by various parameters such as voltage, pulse duration and number of pulses. When all settings match the geometry of the prostate and tumor (always allowing for a safety margin around the tumor), NanoKnife charges its capacitors.
A potential difference builds up between each set consisting of two needles each. This is normally 3000 volts (V). This means that there is +1500 V on needle 1 and -1500 V on needle 2. The patient remains at 0 V. These voltages may seem more life-threatening than gentle, but their duration of action is in the range of millionths of a second. This makes the procedure safe and side effects such as burns are avoided. For more on the technology and the theory behind it, read more about the theory of IRE here.
The number of needles may vary and depends largely on the area to be treated. The computer of the NanoKnife system takes over the appropriate control of the needles, according to the previous settings. The treatment itself usually takes only seconds, a few minutes at most.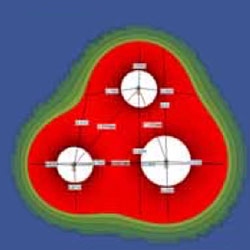
Figure 2: Precise planning of IRE treatment
Immediately after the needles are pulled out, the puncture sites close again. Most patients do not experience pain. However, some find the bladder catheter that is placed prior to treatment uncomfortable. It can be removed after 10 to 14 days. Small amounts of blood may still be found in the urine or seminal fluid several weeks later. This is because it takes up to six months for the body to move the tissue destroyed by NanoKnife ablation out of the body.
How good is IRE
compared to
radical prostatectomy (RPE)?
Evaluation of results from 471 IRE treatments.
While we have successfully treated nearly 1300 men with prostate cancer at the VITUS Prostate Center in the meantime (as of March 2021), we have published the results of 471 IRE treatments over a maximum observation period of 7 years².
Table 2 shows that the majority of the patients we treated suffered from high-risk prostate cancer according to the D’Amico classification.
Table 2
Most of the carcinomas were in stage T2a to T2c, i.e. within the prostate and had not yet (macroscopically) broken through the prostate capsule (“organ confined disease”). However, 84 patients with T3 and T4 carcinomas were also treated, i.e. carcinomas that had already penetrated the prostate capsule and spread outside the prostate (“non-organ confined disease”). Our treatment successes clearly show that IRE is not only suitable for the treatment of early, small carcinomas but also for the treatment of advanced carcinomas.
T4 N0 M1 /
T4 N1 M1
Table 3
During the observation period of 70 months, only 4 recurrences occurred in patients with low-grade Gleason 6 carcinomas, 15 recurrences in patients with intermediate-grade Gleason 7 carcinomas, and 22 recurrences in the patient group with high-grade Gleason 8-10 carcinomas. Comparison with recurrence rates after radical prostatectomy (RPE) as specified in the Johns Hopkins University Han Tables shows that recurrence rates after IRE are comparable to those after RPE.
Recurrence rates after
IRE treatment
(NanoKnife)
Comparable to recurrence rates after radical prostatectomy
How can this be? After the radical removal of the prostate, the cancer should be completely removed from the body after all. But it is not so.
Looking more closely at the HAN Tables, one finds that recurrence rates after radical prostatectomy are high even when the tumor was completely removed along with the prostate (“organ-confined disease” category). So where do the recurrences in these cases come from? They originate from individual tumor cells that have migrated out of the prostate along connective tissue structures, lymphatic and blood vessels and have become embedded in the connective tissue surrounding the prostate. In fact, the tumor cells also circulate in the blood and can be detected there by means of a liquid biopsy.
This is because the prostate capsule is permeable to cells as it consists only of compacted connective tissue fibers. You can imagine it like the edge of a forest: from a distance of 1 km, the edge of the forest looks like a wall, but when you stand directly in front of it, you notice that it consists mainly of air, with a few branches and tree trunks in between. Accordingly, most recurrences after prostatectomy occur in the connective tissue that surrounded the prostate – and surrounds the prostate analogs after prostate removal.
So, strictly speaking, any prostate cancer treatment is just tumor mass reduction – the destruction or removal of the tumor mass IN the prostate. Tumor cells OUTSIDE the prostate remain in the body. This can be killed by the body’s own immune system. The patient is then cured – by his own immune system.
Therefore, it is not too surprising that recurrence rates after IRE treatment are comparable to recurrence rates after prostatectomy and radiotherapy.
Table 5 shows the number of recurrent tumors in the observation period of maximum 70 months in the different Gleason Score groups in 471 IRE treatments performed at VITUS Private Clinic. As expected, most recurrences occurred in the aggressive prostate cancer group (Gleason 8 -10). Fewer recurrences occurred in the Gleason 7 group and the fewest in the Gleason 6 group.
Number of recurrent tumors, total N = 41/429, at max. 70 months follow-up
Table 4

The graph in Figure 1 shows the Kaplan-Meier curves of the 471 IRE treatments evaluated. The Kaplan Meier curves show the number of patients who developed prostate cancer recurrence in a given period after IRE treatment, again divided by prostate cancer aggressiveness: Gleason 6, Gleason 7, and Gleason 8-10. The maximum observation period was again 70 months.
It is interesting to compare the recurrence rates of the aggressive carcinomas (red curve) with the recurrence rates after radical prostatectomy (RPE) as obtained from the Han Tables of Johns Hopkins University, USA (blue and pink dashed lines). The comparison was made with data from patients with comparable tumor stage and Gleason score. Recurrence rates after IRE treatment (red curve) are in the “corridor” of recurrence rates after radical prostatectomy – i.e., they are comparably high.
The distinction between the different localizations of recurrences is also interesting: overall, only 8 of the 41 recurrences occurred within the IRE ablation field, and 15 occurred directly adjacent to the IRE field.
These can be assumed to have surviving tumor cells within or just outside the ablated tumor focus. However, 16 of 41 “recurrences” occurred in regions of the prostate that had been assessed as “tumor-free” prior to treatment and therefore had not been treated. Thus, these were small and minute carcinoma foci that had not attracted diagnostic attention, mainly in patients who had not undergone extensive diagnostic workup prior to IRE treatment: these patients refused 3D mapping biopsy (3DMB) and/or optimal endorectal MRI and/or PSMA-PET/CT with gallium68. In the strict sense, these “recurrences” are therefore not recurrences at all, but additional tumor foci in the prostate that were not known.
If these “pseudo-recurrences” are removed from the statistics and the Kaplan-Meyer curves are calculated based on the actual recurrences, even longer recurrence-free survival times are achieved. This can be seen in graph X: The Kaplan-Meyer curve for recurrence-free survival is shifted upward (gray arrows).

One ablation zone was generated per electrode pair (red ellipses). In the image after contrast administration, the ablation zone is clearly visible as an avascular area without blood supply. PSA levels decreased from 5.2 ng/ml before treatment to 2.3 ng/ml after IRE, rather than zero, because the right prostate lobe was preserved. This is typical of focal therapies.
IRE in prostate cancer:
High efficacy – low side effects
The table below shows side effects that occurred during the treatment of 471 prostate cancers at the VITUS Prostate Center.
First, it is noteworthy that due to the minimally invasive treatment, no life-threatening side effects and no deaths occurred.
Mild side effects occurred in approximately 1/5 of IRE-treated patients (green boxes), such as transient difficulty with urination (urine retention), so that a new urinary catheter had to be inserted after removal of the first bladder catheter and left in the bladder for a further 10-14 days. Mild discomfort and/or pain during urination (dysuria) and mild blood in the urine (hematuria) occurred in approximately 7% and 4% of patients, respectively.
Moderately severe adverse events occurred in only 2.5% of IRE-treated patients (yellow boxes). These were urinary tract infections due to the catheter, which had to be treated with antibiotics.
Medically relevant adverse events, but not life-threatening, occurred in only 1.3% of IRE-treated patients (pink boxes). These were persistent problems with urination caused by dead tumor tissue in the prostate, which had to be treated by removal of the tissue via the urethra (TURP), a fistula between the rectum and the prostate caused by the treatment, which healed spontaneously, and a perforation of the bladder caused by a urinary bladder catheter, which also closed spontaneously.
Clinical or diagnostic monitoring only – no treatment required
(19.5%)
(9.0%)
(6.7%)
(3.8%)
Minimal, local or non-invasive treatment indicated; restriction of age-appropriate activities of daily living
(2.5%)
(2.5%)
(0.8%)
(0.8%)
(0.2%)
(0.2%)
Urgent medical measures required
Table 5
Incontinence prevention
Zero percent incontinence rate after IRE treatment in well over 1000 patients.
Incontinence is a common and serious side effect in approximately 50% of men who have undergone radical prostatectomy – with or without daVinci robots. Incontinence is difficult to avoid during surgical removal of the prostate, because the bladder sphincter (also called lower urinary sphincter – LUS) is located directly below the prostate and protrudes into the apex, the lower part of the prostate. If the prostate is removed, part of the sphincter is also removed. Further damage to the LUS occurs when the base of the bladder is sutured down after the prostate is removed and sutured to the sphincter muscle to ensure urine flow.
No incontinence has occurred in the more than 2000 patients treated with IRE to date. This fact was easy to ascertain because treated patients report it immediately, even with only minor involuntary urine loss. And indeed, immediately after IRE treatment, a small percentage of patients experience transient incontinence due to two mechanisms:
- The dilatation of the sphincter muscle by the catheter, which remains in the urinary bladder for 10 to 14 days.
- Urge incontinence”, which occurs due to irritation of the prostate gland after tumor destruction (as is also the case with prostatitis) and is noticeable in that affected men feel a sudden urge to urinate when the bladder is full and lose urine on the way to the toilet.
These types of incontinence are temporary and regress after a few days to a maximum of 3 months. They have nothing to do with the irreparable destruction of the sphincter muscle that occurs after surgery.
Table 6 shows our published data on urinary incontinence:
Table 6
Erectile dysfunction prevention
Zero to maximum 10% impotence after IRE treatment for prostate cancer.
The neurovascular bundle (NVB), a network of nerves and vessels, is responsible for the erketion function of the penis. It is mostly located inside and directly on the prostate capsule (see Figure 2) and therefore cannot be preserved during either radical prostatectomy or radiotherapy.
Therefore, the actual impotence rates after conventional prostate cancer treatment are very high at 60-90%, even after a so-called “nerve-sparing prostatectomy”. The result is the loss of erectile function: impotence.

Irreversible electroporation (IRE – NanoKnife) as a “problem solver” in inoperative prostate cancer: rectal infiltration, bladder floor infiltration, sphincter infiltration.
The treatment was performed with 5 electrodes whose positions are visible the day after the treatment (small black circles). One ablation zone was generated per electrode pair (red ellipses), for a total of 9 individual ablation zones. In the image after contrast administration, the total ablation zone is clearly visible as an avascular area without blood supply.
The prostate tissue was completely destroyed, only the prostate capsule is preserved, as it is largely composed of connective tissue, which is not destroyed by IRE. The PSA level decreased to 0 ng/ml, as after prostatectomy.

PSA 11 ng/ml


PSA 0.0 ng/ml
The figures show the treatment of a prostate carcinoma stage T2c, N0, M0, Gleason score 8, in a 63-year-old man. The carcinoma has spread over both lobes of the prostate. In this case, focal therapy with preservation of substantial portions of healthy prostate tissue was no longer possible.
“Radical” therapy of prostatic carcinoma with Irreversible Electroporation (IRE – NanoKnife) – complete ablation of the prostate.
Figure 3 shows the treatment of a prostate carcinoma stage T4, N0, M0, Gleason score 8, in a 79-year-old man with infiltration of the rectum (rectal area; yellow arrows above). Radical prostatectomy would have been possible only with additional removal of the rectum and creation of an artificial anus praeter.
Infiltration of the rectum is shown on the MRI images in the top row of Figure Z: Left: lateral (sagittal) image; Middle: cross-sectional (axial image) with T2 weighting; Right: cross-sectional (axial image) after contrast administration.
The lower row of images shows the conditions 9 months after IRE treatment: The wall of the rectum appears normal, without injury and without fistula (malconnection) to the prostate: Left: lateral (sagittal) image; Middle: cross-section (axial image) with T2 weighting; Right: cross-section (axial image) after contrast administration.


Inoperable prostate carcinomas:
Often not detected due to inadequate diagnostics
In the meantime, we have successfully treated dozens of patients with inoperable prostate carcinomas at the VITUS PRIVATKLINIK, preserving their function. If you suffer from advanced prostate cancer, let our experts advise you.
Unfortunately, inoperable tumor stages are often not detected before surgical intervention because sufficiently accurate diagnostics have not been performed.
This leads either to the abortion of the operation or to the incomplete removal of the tumor, in some cases also to the removal of the bladder and the rectum together with the prostate and, among other things, to the creation of an artificial outlet for the intestine and the bladder. In many cases, such a disaster can be avoided.
